THE NATURAL HISTORY OF AIDS By Roberto Giraldo
June 2000
Coincidentally, AIDS appeared in distant and various areas of the Earth during the second half of the 20th century, at a moment when the immune systems of humans, as well as other bodily systems, were already saturated with exposures to a great variety of stressor agents (1-3). In AIDS the immune system is devastated, it is collapsed. All other bodily systems are also suffer the consequences of the exposure to stressors.The capabilities and possibilities of the immune system are neither infallible nor infinite. They have limits. AIDS is the maximum state of deterioration that the human immune system can reach. If the pathogenic process of AIDS is not stopped, eventually it will kill the person (4-7).
Currently, everybody’s immune system is being challenged by the worldwide increment in immunological stressor agents of chemical, physical, biological, mental, and nutritional origin. However, the diversity and intensity of these risks or etiologic factors for AIDS vary from person to person, from group at risk to group at risk, from country to country, and from continent to continent. This is the principal reason why the frequency of AIDS is not homogeneous in all places and countries (1-3).
If immunological stressors continue to increase in number and strength and if they spread to new social groups, as will probably happen, the number of people at risk for AIDS will rise. Obviously, this is influenced by the diversity, quality and quantity of the stressors, route of exposure, duration and dose, as well as by individual and group susceptibilities (1-3).
The most important risk factor for AIDS in developed countries is the new epidemic of drugs abuse (Duesberg 92; Duesberg & Rasnick 98). The most important risk factor for AIDS in underdeveloped countries is poverty, with all its consequences: malnutrition, unsanitary conditions, infections, parasites, and lack of hope for a better life, all of which have reached unprecedentedly high levels in the last few decades (4-7).
1. Proposal for Grading Exposures to Etiologic Factors for AIDS Within Developed and Underdeveloped Countries
Immunological stressors, also known as "co-factors", are the real risk, etiologic or causal factors for AIDS (4-7). Multiple, repeated, and chronic exposure to immunological stressors of chemical, physical, biological, mental, and nutritional origin are the risk factors for reacting positively on the tests for HIV and for developing AIDS (8-13).
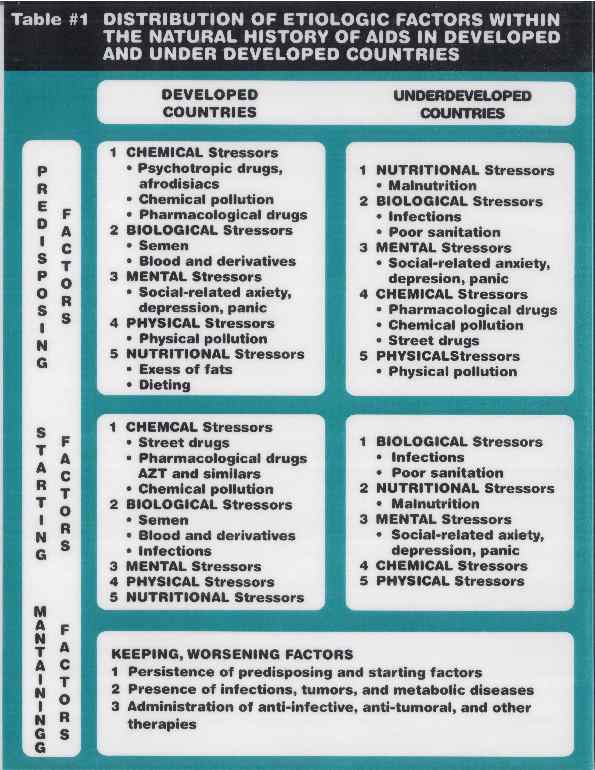
Immunological stressors can weaken the immune system, predisposing the individual to AIDS, i.e., stressors can constitute predisposing factors. In a person with a debilitated immune system the exposure to more immunological stressors can determine the beginning of the disease, i.e., starting factors. And in a person already sick, the continuation of exposures to stressors keeps or worsens the sickness status ¾ keeping/worsening factors ¾ which eventually brings death (5,7).
Table #1 shows the distribution of the etiologic factors for AIDS within developed and underdeveloped countries.
The primary predisposing factors for AIDS in developed countries are chemical in origin, such as recreational drugs (cocaine, heroine, marijuana, alkyl nitrites, met amphetamines), the chemicals polluting the air, water, and soil, the chemicals used in food preservation, and pharmaceutical medications (14-18). Secondary predisposing factors are biological stressors such as semen through anal intercourses (8,9,19), and blood and derivatives in hemophiliacs and other patients treated with transfusions (20,21). Mental stressors are the third group of factors that can weaken the immune system in these countries (22-25). Anxiety, depression, and periods of panic, secondary to social conditions such as prostitution, drug-addiction, the knowledge of being "HIV-positive", hemophilia, homophobia, AIDS-phobia, lack of hope for a better life, are the main mental stressors (22-25). Then come the physical pollutants such as noise, electromagnetic fields, along with ionizing and non-ionizing radiations (26). The excess of fats as well as diets lacking in certain nutritional needs may constitute a fifth group of AIDS predisposing factors in developed countries (27,28).
In underdeveloped countries, by contrast, the most important factor debilitating the immune system is the lack of nutritional needs, which starts in fetal life (29) and accompanies people throughout their lives (30). Secondary factors are biological stressors such as infections and parasitosis due to poor sanitation conditions (biological pollution) (31). Further factors are social and mental stressors brought on through a lack of hope for a better life, a hopelessness which also weakens immune systems in these countries (22-25). A fourth level of stressors would be chemical stressors, but in the poorer countries drugs from the conventional pharmacopoeia (antibiotics and anti-parasites) contribute more than recreational drugs (14). Industrial chemical and physical pollution can also be predisposing factors to AIDS, principally for people living in the large cities of the underdeveloped countries (32).
The more common etiologic factors that permit AIDS to start (starting factors) in developed countries are again the recreational drugs (15-18). Pharmacological medicines such as AZT and other chemicals from environmental pollution can also often be the switch which starts AIDS (15,16,33). The immunodepressive effects of semen, blood and derivatives can also act as starting factors (19-21). Certain infections such as viral hepatitis, herpes simplex, herpes zoster, syphilis, and gonorrhoea can act as starting factors in people with already weakened immune systems (31). The same can happen with an acute crisis of anxiety, depression or panic in debilitated individuals (22-25). The mere fact of knowing oneself to be "HIV-positive" is a strong immunological stressor (22-25). Less frequently in industrialized countries, the exposure to physical and nutritional stressors can turn an asymptomatic state ¾ "HIV-positive" ¾ into a symptomatic disease (28,34).
The most frequent starting factor for AIDS in underdeveloped countries is a new infection or parasitosis in a previously malnourished and debilitated host (31,35,36). A specific nutritional deficiency can also be a starting factor (28,34). Also, a mental stressor (22-25), and, less frequently, a chemical such as alcohol or a physical stressor can be the one that switches on the disease (14-16).
In both type of countries, the factors that maintain the disease status, or can worsen the course of AIDS, are the persistence of the predisposing and starting factors, the presence of infections, tumors, and metabolic diseases, as well as anti-infective, anti-tumoral, and anti-retroviral therapies with potential immunotoxic and immunodepressive properties. Interestingly, there are three vicious circles during the course of AIDS:
immunodeficiency = infections = more immunodeficiency
immunodeficiency = neoplasias = more immunodeficiency
immunodeficiency = metabolic diseases = more immunodeficiency
It should be emphasized that the etiologic factors for AIDS, for people living in the expanding impoverished areas of the big cities in developed countries ¾ "thirdworldization" ¾ are very similar to those of underdeveloped countries (1-3).
It is also important to point out that malnutrition in underdeveloped countries and the use of street drugs in developed ones during pregnancy are etiologic factors for children born with AIDS (13,15,16).
Therefore, the etiologic factors for reacting positively on the tests for HIV and for developing AIDS apply to all persons developing the syndrome, everywhere: to drug addicted gay men; IV drug users; non IV drug users and alcoholics; prostitutes; babies born to drug users or malnourished mothers; hemophiliacs; people with strong AIDS-phobia; African, Asian, Caribbean, and similar people; African-Americans and Hispanics in the USA; as well as to those people getting AIDS from occupational exposures to immunological stressors and to those who develop AIDS secondary to the prescription of anti-retrovirals.
2. Role of Tropical Diseases in AIDS
In Africa, Asia, the Caribbean and similar communities, malnutrition and other conditions due to poverty, also known as "tropical diseases", have important roles as predisposing, starting, and continuing factors for reacting positively on the tests for HIV and for developing AIDS (4,7,8,13).
The mechanisms by which malnutrition, tuberculosis, sexually transmitted diseases, malaria, trypanosomiasis, schystosomiasis, leishmaniasis, systemic mycosis, as well as other infections and parasites weaken, destroy, and collapse the immune system are well known. These mechanisms should be emphasized in any attempt to understand the current occurrence of the AIDS epidemic in the poorest areas of the underdeveloped countries (31,35-39).
To understand this issue and its full magnitude, it is necessary to comprehend that never before were the poor so poor and so sick as they are now. Recently, the levels of malnutrition, infections, and parasites have reached very alarming levels (40-41).
3. Role of "HIV/AIDS Hysteria" in AIDS
A new risk factor for AIDS, created during the AIDS pandemic, is the belief itself that HIV is the cause of AIDS.
The mere knowledge of being or simply the feeling of being "HIV-positive" is a strong condition that can act by itself as a predisposing, starting, or continuing factor for AIDS.
The issue of mental stress as an immunodepressive agent has been addressed many times in relation to the onset, course, and prognosis of AIDS (22-25).
In order to stop the AIDS epidemic it is absolutely necessary to first end the "HIV/AIDS hysteria." Both in the individual and in the community: the feeling of being infected with the virus that causes AIDS blocks the participation of the brain and mind in the healing process.
Another terrible consequence of the "HIV/AIDS hysteria" is the feeling of rejection toward sexual life, a feeling already experienced by many. Since it is believed that one can get AIDS from having sex even with husbands or wives, the logical conclusion is that sexual intercourse is something dangerous. This misleading information ought to be stopped immediately. It is important to defend the right of people to normal sexual life.
4. Increment of Exposures to Immunological Stressors in People at Risk of AIDS
It should be pointed out that in addition to the broad spread of environmental pollution in recent decades, people who react positively on the tests for HIV or who develop AIDS are being challenged by many other immunological stressors or oxidizing agents prior to the onset of the syndrome (8-13).
Following is a proposal for the distribution of exposures to immunological stressors ¾ the risk or etiologic factors for AIDS ¾ within the different groups of people at risk to react positively on the tests for HIV and to develop AIDS (1-3).
4.1. Drug addicted gay men:
- Alcohol and drugs of abuse (chemical stressors)
- STD's (biological Stressors)
- Other infections (biological stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressors)
- Sperm (biological stressor)
- Mental distress (mental stressors)
- Malnutrition (nutritional stressor)
4.2. IV drug users:
- Alcohol and drug abuse (chemical stressors)
- Blood borne infections (biological stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressors)
- Mental Distress (mental stressors)
- Malnutrition (nutritional stressors)
4.3. Non-IV Drug users and alcoholics:
- Alcohol and drug abuse (chemical stressors)
- Opportunistic infections (biological stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressors)
- Mental Distress (mental stressors)
- Malnutrition (nutritional stressors)
4.4. Prostitutes:
- Alcohol and other drugs (chemical stressor)
- Sperm (biological stressor)
- STD’s (biological stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressors)
- Mental Distress (mental stressors)
4.5. Babies born to drug abuser mothers:
- Alcohol and drug abuse during pregnancy (chemical stressors)
- Congenital infections (biological Stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressor)
- Fetal malnutrition (nutritional stressors)
4.6. Babies born to malnourished mothers:
- Congenital infections (biological Stressors)
- Fetal malnutrition (nutritional stressors)
4.7. Hemophiliacs:
- Blood and factor VIII (biological stressors)
- Infections (biological stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressors)
- Mental Distress (mental stressors)
4.8. AIDS-phobic people:
- Mental Distress (mental stressors)
- Medications for prevention including anti-retrovirals (chemical stressors)
4.9. African Asian, the Caribbean, and similar communities:
- Malnutrition (nutritional stressors)
- Infections and parasites (biological stressors)
- Anti-infective therapy (chemical stressors)
- Mental distress (mental stressors)
4.10. African-Americans and Hispanics in USA:
- Mental distress (mental stressors)
- Malnutrition (nutritional stressors)
- Alcohol and other drugs (chemical stressors)
- Anti-infective therapy including anti-retrovirals (chemical stressors)
4.11. Occupational-related Risk Group:
- Environmental/occupational chemical pollution (chemical stressors)
- Electromagnetic fields and other radiations (physical stressors)
- Infectious agents (biological stressors)
- Diets (nutritional stressors)
- Mental distress (mental stressors)
4.12. Iatrogenic group:
- Medications for prevention including anti-retrovirals (chemical stressors).
- Mental distress (mental stressors)
5. Proposal for the Natural History of AIDS
Being that AIDS is the same condition everywhere, it may have a common natural history in all people suffering from it. What changes from patient to patient and from country to country is the type and dose of the etiologic factors, which are in this case the immunological stressors (1,2,4-6,8). Therefore, as happens with any other human condition caused by external agents, when doing a diagnostic analysis of AIDS, the etiologic factors should be searched and graded for each individual, group of people, country, and group of countries.
Graph #1 shows my proposal for the natural history of AIDS.
Light, moderate, or severe acquired immunodeficiency [8] is a consequence of immunogenic [6] and immunotoxic [7] degenerative effects upon immune cells and immune metabolic reactions from multiple, repeated, and chronic exposures to immunological stressors [1,2,3,4,5]. During the course of a severe acquired immunodeficiency, like the one that occurs in AIDS, all three main functions of the immune system become deficient: defense [9], homeostasis [10], and surveillance [11].
Certain infectious agents [12] find in the weakening of the defense functions [9] a unique opportunity to grow, generating a variety of opportunistic infections [15]. The deficiency in the homeostasis functions [10] is responsible for the diversity of metabolic diseases [16] seen in AIDS patients. The deficiency of the surveillance functions [11], together with the presence of specific carcinogenic agents [13], and other factors involved in the carcinogenesis process, are responsible for the occurrence of neoplasias [17]. Obviously, the simultaneous appearance of life-threatening infectious, metabolic, and neoplasic diseases depends besides the type and dose of the immunological stressors and on the physiological status [14] of the individual, given by many variables such as age, gender, personality, nutrition, pregnancy, lactation, detoxification status, responsiveness of tissues, and genetics.
If the exposure to immunological stressors is not stopped, and/or if the patient is medicated with anti-infective, anti-tumoral, and anti-retroviral therapies [18,19] a greater stage of immunodeficiency comes, with an increment in metabolic alterations and nutritional needs [20]. This brings the patient into a stage of severe malnutrition and generalized metabolic disturbances [21], with an increasing hazard of death [22].
The reactivity on the tests for HIV that occurs beginning in the earlier stages of the natural history of AIDS ¾ stages without clinical manifestations ¾ may be part of the stress response of the individual to multiple, repeated and chronic exposure to immunological stressor or oxidizing agents (8-13).
This article was written in June 2000 and posted during the Internet Discussion of the South African Presidential AIDS Advisory PanelReferences
- Giraldo RA. AIDS and Stressors I: Worldwide Rise of Immunological Stressors. Toxicology Letters Supplement 1/78. 1995: s34.
- Giraldo RA. AIDS and Stressors I: Worldwide Rise of Immunological Stressors. In: AIDS and Stressors, Medellín: Impresos Begón, 1997: 23-56.
- Giraldo RA. El Alarmante incremento mundial de Agentes Estresantes Inmunologicos. In: Ahumaca C. tet al. Relaciones Internacionales, Politica Social y Salud: Desafios en la Era de la Globalizacion. Bogotá: Fundación Cultural Javeriana, 1998: 49-73.
- Giraldo RA. AIDS and Stressors II: A Proposal for the Pathogenesis of AIDS. Toxicology Letters Supplement 1/78. 1995: s34.
- Giraldo RA. AIDS and Stressors III: A Proposal for the Natural History of AIDS. Toxicology Letters Supplement 1/78. 1995: s35.
- Giraldo RA. AIDS and Stressors II: A Proposal for the Pathogenesis of AIDS. Stressors. In: AIDS and Stressors, Medellín: Impresos Begón, 1997: 57-96.
- Giraldo RA. AIDS and Stressors III: A Proposal for the Natural History of AIDS. In: AIDS and Stressors, Medellín: Impresos Begón, 1997: 97-131.
- Papadopulos-Eleopulos E. Reappraisal of AIDS – Is the Oxidation Induced by the Risk Factors the Primary Cause? Medical Hypothesis 1988; 25: 151-162.
- Papadopulos-Eleopulos E. Looking Back on the Oxidative Stress Theory of AIDS. Continuum (London) 1998/9; 5(5): 30-35.
- Papadopulos-Eleopulos E et al. Oxidative Stress, HIV and AIDS. Res Immunol 1992; 143: 145-148.
- Papadopulos-Eleopulos E et al. Is a Positive Western blot Proof of HIV Infection? Bio/Technology 1993; 11: 696-707.
- Papadopulos-Eleopulos E et al. The Isolation of HIV: Has it Really Been Achieved? The Case Against. Continuum (London) September/October 1996; 4(3): s1-s24.
- Giraldo RA et al Is it Rational to Treat and Prevent AIDS with Toxic Antiretroviral Drugs in Pregnant Women, Infants, Children, and Anybody Else? The Answer is Negative. Continuum (London) 1999; 5(6): 38-52.
- Descotes J. Immunotoxicology of Drugs and Chemicals. Amsterdam: Elsevier; 1988.
- Duesberg PH. AIDs Acquired by Drug Consumption and other Noncontagious Risk Factors. Pharmac Ther 1992: 201-277.
- Duesberg PH, Rasnick D. The AIDS Dilema. Drug Diseases Blamed on a Passenger Virus. Genetica 1998; 104: 85-132.
- Specter S. Bendinelli M Friedman H. Drugs of Abuse, Immunity and AIDS. New York: Plenum Press; 1993: 300.
- Friedman H et al. Drugs of Abuse, Immunity and Infection. New York: Plenum Press; 1995: 350.
- Root-Bernstein RS, Hobbs de Witt S. Semen Alloantigen and Lymphocytotoxic Antibodies in AIDS and ICL. Genetica 1995; 95: 133-156.
- Duesberg PH. Foreign-Protein-Mediated Immunodeficiency in Hemophiliacs with & without HIV. Genetica 1995; 95: 51-70.
- Papadopulos-Eleopulos E et al. Factor VIII, HIV and AIDs in Hemophiliacs: An Analysis of their relationship. Genetica 1995; 95: 25-50.
- Kemeny ME. Psychoneuroimmunology in HIV Infection. In: Zegan LS & Coates TJ. Psychiatric Manifestations of HIV Disease. The Psychiatric Clinics of North America. Philadelphia: Saunders Co. 1994: 55-68.
- Glaser R, Kiecolt-Glaser JK. Handbook of Human Stress and Immunity. San Diego: Academic Press, 1994.
- Kiecolt-Glasser JK & Glaser R. Psychological Influences in Immunity. Implications for AIDS. Amer Psychologist 1988; 43: 892-898.
- Schneiderman N, et al. Psychoneuroimmunology and HIV/AIDS. In:Schedlowski M & Tewes U. Psychoneuroimmunology. New York: Kluwer Acadamec /Plenum Publishers. 1999: 487-508.
- Gold. JM. The Enemy Within. The cost of living near nuclear reactors. Breast Cancer, AIDS, Low Birthweights, and other Radiation-induced Immune Deficienciy defects. New York: Four Walls Wight Windows; 1996: 346.
- Chandra RK. Nutrition and Immunity: Lesons from the Past and New Insights into the Future. Amer J Clin Nutr 1991; 53: 1087-1101.
- Hickson JF. Diet and Nutrition for Optimal Immune Function. In: Bahl SM, Hickson JF. Nutitional Care for HIV-Positive Persons: A Manual for Individuals and Their Caregivers. Boca Raton: CRC Press, 1995: 1-36.
- Chandra RK. Fetal Malnutrition and Postnatal Immunodeficiency. Am J Dis Chil 1975; 125: 450-455.
- Chandra RK. Interactions Between Early Nutrition and the Immune System. In: Barker DJL & Whelan J. The Childhood Environment and Adult Disease. Siba Foundation Symposium 156. London: Wiley; 1991: 77-88.
- Cunningham MW, Fujinami RS. Effects ob Microbes on the Immune System. Philadelphia: Lippincott Williams & Wilkins; 2000: 662.
- Fischbein A, Tarcher AB. Disorders of the Immune System. In: Tarcher AB. Principles and Prectice of Environmental Medicine. New York: Plenum Medical Book, 1992: 389-411.
- Lauritsen J. Poison by Prescription: the AZT Story. New York: Asklepios, 1990.
- Chandra RK. Nutrition, Immunity and Infection.: Present Knowledge and Future Directions. Lancet 1983; 1: 688-691.
- Ware RE, Kline MW. Immunodeficiency Secondary to Infectious Diseases. In: Rich HH, et al. Clinical Immunology: Principles & Practice. St. Louis: Mosby; 1996: 808-826.
- Nusseinzweig RS. Parasitic Disease as a Cause of Immunossuppression. NEJM 1982; 306: 423-424.
- Jain VK & Chandra RK. Does Nutritional Deficiency Predispose to Acquired Immunodeficiency Syndrome? Nutr Res 1984; 4: 537-542.
- Lamoureaux G et al. Is Prior Mycobacterial Infection a Common Predisposing Factor to AIDS in Haitians and Africans? Ann Inst Pasteur/Immunol 1987; 138: 521-529.
- Cates W Jr. The "Other STD’s" Do They Really Matter? JAMA 1988; 259: 3606-36-08.
- World Health. Reaching out to the poorest. World Health: Magazine of the World Health Organization. 1994; 47: 1-31.
- World Bank. Confronting AIDS: Public Priorities in a Global Epidemic. A World Bank Policy Research Report. 1999: 365.